Hits: 317
Reprinted with permission. March 8, 2023
The House Select Subcommittee on the Coronavirus Pandemic has started to convene on everything from COVID-19 origins to vaccines. Last week, they called in four scientists to discuss policies, including lockdowns.
COVID-19 control measures are important to discuss. We still don’t know what policies worked best and why.
Pandemic health protections had benefits AND harms. There were trade-offs, just like with any health policy. Governments around the world used a wide variety of policies before vaccines were developed.
However, a nuanced discussion of the trade-offs inherent in pandemic control measures was not achieved last week. The Great Barrington Declaration (GBD), for example, dominated the conversation.
It looks like we are entering a new phase of the pandemic—revisionism.
Great Barrington Declaration
In October 2020, the GBD advocated for a distinct approach: isolate the vulnerable while allowing infections to spread among lower-risk members of the population. It claimed this would ultimately achieve herd immunity without the economic and social toll of lockdowns.
The authors of the GBD didn’t include any scientific evidence or models, and it was never peer-reviewed.
The idea went viral. A few influential people listened. Trump met with the GBD authors in the Oval Office. Trump’s coronavirus czar, Scott Atlas, embraced and adopted the GBD—for example, he successfully curbed federal testing programs. Florida governor Ron DeSantis was advised by the GBD. But scientific consensus rejected the idea.
Two of the GBD authors were invited to testify last week. One congresswoman said: “History is proving [them] to be right.” But were they right?
The committee would have benefited from looking into the scientific evidence against the GBD and why, ultimately, public health dismissed their ideas.
Epidemiological problems with GBD
Last year mathematicians published epidemiological models to answer the question: What would it have looked like if we had actually deployed the GBD?
They found that in a town of 1 million people in England:
- Doing nothing (i.e. no shielding of the vulnerable) would have resulted in 415 deaths per 100,000—equivalent to 230,795 total deaths in England.
- This is likely a conservative measure, given that the model didn’t take into account the collapse of healthcare.
- “Perfect shielding” (i.e. the GBD approach) would have resulted in 87.6 deaths per 100,000—equivalent to 50,000 total deaths among younger populations.
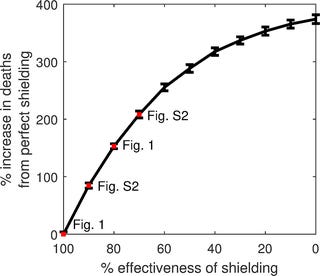
So, in theory, perfect shielding would save lives compared with no shielding. But theory is very different from practice. There are three major issues:
- It is impossible to 100% shield vulnerable adults. In England, 3 in 4 vulnerable people live with other people. There is no “them,” there is only “us,” so shielding them would not be perfect. If shielding had been 80% effective (instead of 100%), the researchers found that there would be massive outbreaks among the vulnerable, resulting in 221.7 per 100,000 deaths. Shielding entire populations worked in some countries in the short term (averting mass death, hospitalization, and orphanhood). It also worked in some Alaskan villages in the 1918 flu pandemic. But trying to shield sub-populations would spark superspreader events. Research shows that infection in younger people led to infections and deaths in older people.
- The GBD relied on large numbers of lower-risk individuals becoming infected to build up immunity in the population, yet many people would have likely still changed their behavior to avoid getting infected and sick. Even before England’s first lockdown, there were dramatic changes in behavior—people voluntarily reduced their contact with others. And if health services had been under strain, people would probably have reduced their contacts even further. This would make it even harder to reach herd immunity.
- Herd immunity from infection would only have conferred indirect, temporary protection to the shielded vulnerable people. We see this today—although a large proportion of the population has immunity, older adults are still vulnerable to death.
Ethical and logistical problems with GBD
The modeling above assumes that it is actually logistically possible in the U.S. to somehow isolate tens of millions of Americans. This assumption has problems:
- How would we have rapidly and accurately identified “the vulnerable”? The U.S. doesn’t have a universal healthcare system or registry.
- How would we have cared for so many isolated people for such a long time? This would have been a LOT of people. Where exactly would they have gone? The GBD made some vague suggestions about “empty hotel rooms.” Did we really have enough rooms for around 100-130 million people?
- What about long COVID-19 among the population with infections?
The need for better discussion
Many countries regrouped after the 2003 SARS pandemic, and it was incredibly helpful for their future preparedness and response. We do need to reflect on what went right during the pandemic, what went wrong, and how to do better in the future, like:
- Did some states do better than others? What does “better” mean?
- What steps should states have taken to mitigate the harms of shelter-in-place orders? Why didn’t all states provide generous food, social, and financial support to those living under such orders?
- What is the decision framework for closing and reopening schools in future pandemics?
The discussion has to be serious, genuine, and balanced.
Thus far, this has not been the case.
It’s clear that achieving a healthier and smarter future isn’t the goal of this Subcommittee.
We should be very wary of those trying to rewrite history. As Zeynep Tufecki said:
“There’s an attempt to relitigate 2020 under the comfort of 2023 vaccines, treatments, [and] population immunity by people… whose policy suggestions were catastrophically wrong. They’re pretending 2023 exonerates the deaths they would cause (did cause). I find that awful.”
This Subcommittee is a huge use of resources, which, thus far, has not helped move the conversation forward. The outcome of these rabbit holes do not get us to a better place.
Bottom line
We need to learn lessons from the pandemic to be better and smarter next time.
But discussions need to be balanced and informed. For example, recognizing the trade-offs must include recognizing the horrors of uncontrolled transmission. Epidemiological, ethical, and logistical details can’t be left out.
Can we please have a serious conversation about the COVID-19 pandemic and how to prepare for the future? Our lives depend on it.
Love,
YLE and GMY
Dr. Gavin Yamey is a Professor of Global Health & Public Policy at Duke University and Director of the Center for Policy Impact in Global Health.
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, data scientist. During the day she works at a nonpartisan health policy think tank and is a senior scientific consultant to a number of organizations, including the CDC. At night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well equipped to make evidence-based decisions. This newsletter is free thanks to the generous support of fellow YLE community members. To support this effort, subscribe below:
Subscribed