Hits: 241

WPCNR Your Local Epidemiologist. Reprinted with permission. August 3, 2022:
There is substantial concern about monkeypox (MPV) exposure and risk among the general public.
Some of this is warranted; some is not.
Misconceptions are taking hold given the rapidly evolving situation and scientific uncertainty.
This post triangulates historical context, lab data, and epidemiological data to show you what we do (and do not) know about MPV transmission right now.
Transmission
In 2019, researchers found that the R(t) of MPV ranges from 0-3. In other words, for every infected person, on average, that person will infect 0 to 3 other people. This was highly dependent on immunity in a population—the more people without immunity, the faster it spread. As of July 2022, the WHO estimates R(t)=1.29. This is pretty low. (For reference, the R(0) of smallpox = 3.5-6, and Omicron is higher.)

We don’t know why MPV is less contagious than other viruses: What is the virus receptor? Does the virus enter the cells more slowly? Is it less “sticky” and not latching on well?
In very broad terms, it’s clearly not as well adapted to infect humans as other viruses. In 2017/2018, MPV substantially mutated (as viruses do). It may have mutated to become more “fit” for human infection, or it may not have. We don’t know yet.
Regardless, because of the lower contagiousness, we hypothesize that we need a higher “dosage” of virus to become infected and sick.
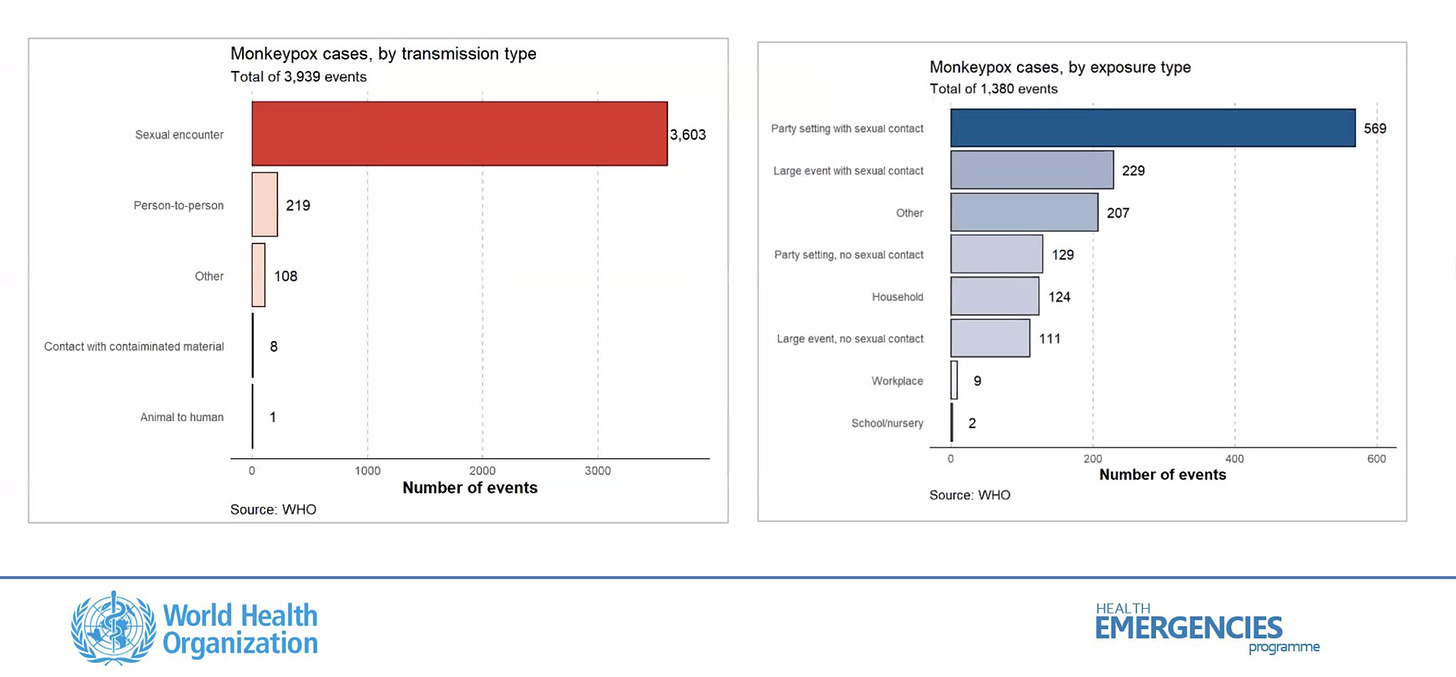
Contact tracing data confirms this, thus far, by showing clear patterns of transmission among very close and prolonged contacts, like sexual encounters. This is consistent with data from the original 2017 outbreak in Nigeria.
There is contagious virus in open lesions. Also, yesterday, the Lancet published the first compelling evidence that replicating virus is also found in semen.
We also see fomite transmission in very heavily contaminated areas (someone’s hospital room, someone’s bedroom at home, etc.) where lots of virus has been shedding for a long time.
A recent study found high contamination in two hospital rooms in all places directly touched by MPV patients: bathroom, chairs, cell phones, and even the floor.
In a preprint, UK scientists sampled hospital rooms of isolated MPV patients and found widespread surface contamination (66 positive out of 73 samples).
But there are three things to keep in mind about surface transmission:
- MPV is hardy on surfaces, and left alone it can linger for quite a while, but it is whimpy against soap and UV light.
- The presence of virus does not mean automatic infection. The dose you’re exposed to needs to be high enough to take hold in the body.
- Even if a surface does have the virus, it does not mean it’s replicating—or infectious.
So, if someone quickly touches a doorknob in public, for example, it doesn’t mean you will be automatically infected after you touch that doorknob. And in fact, we aren’t seeing anything like that in the contact tracing data.
Preliminary data also shows droplet or aerosol transmission.
Some MPV cases have lesions in their mouth, so this could, theoretically, be a mode of transmission if you’re closely talking to someone who has an active (e.g., painful) infection for a long duration of time.
This is why people with active MPV and those caring for them are advised to wear masks.
Previous case studies in Nigeria show secondary transmission among nurses caring for MPV patients without PPE.
A preprint from the UK found positive air samples in hospital rooms of infected patients, specifically when nurses were changing bed sheets.
But, just like surface transmission, this isn’t likely to happen by passing someone at the supermarket.
There is preliminary scientific evidence of asymptomatic transmission.
A preprint from Belgium tested a bank of 224 specimens using a PCR for MPV and identified three infections in people who denied having had any symptoms in the weeks before and after the sample was taken.
This was surprising, but only one study. We need consistency across several studies to know the “true rate” of asymptomatic transmission and public health implications.
We don’t currently have a test for asymptomatic transmission, but scientists are working on it.
High risk: Right now vs. in the future
Because of the distinct transmission pattern, MPV has gained a foothold in one specific, tight-knit social network: men who have sex with men (MSM).
This means this group is most at risk *right now,* and public health outreach, policy, and resources are laser focused on this community, rightfully so.
MPV could spread to other social networks. We saw this happen with MRSA in 2008: It started in one network (gay men) and moved to other social networks (like wrestling teams).
There is considerable chatter regarding MPV spread in colleges and schools, which isn’t too far fetched given tight-knit social and sexual networks on campuses.
This doesn’t mean there should be panic, but institutions should absolutely prepare. (Here is guidance on controlling MPV in congregate settings).
Bottom line
Current data shows that MPV transmission can occur in multiple ways, but what is possible is not always probable.
Epidemiological data shows very close and prolonged exposure absolutely dominating transmission networks.
Groups *at risk* should be aware and adjust behaviors according to risk tolerance.