
Hits: 229
WPCNR CORONAVIRUS ROUNDUP. By John F. Bailey From New York State Covid Tracker and Article from National Geographic. APRIL 11, 2021:
From Tuesday, April 6 through Friday April 9, Westchester County lowered the number of new Covid infections to below 3% for the first time in two months.
The 3% of the total 49,789 tested those four days yielded 1,482 covid positive persons, which can still mean 64 new hospitalizations by next week at a 4.3% hospitalization rate.
Previous to those four days, 25,042 people were tested half the 49,789 tested Tuesday, Wednesday Thursday and Friday, (and county persons testing postive had been 4.3% on April 5, 3.7% on April 4 and 3.6% on April 3. On those three days numbers of positive covid persons was 942, which could yield 40 hospitalizations next week added to the 64, meaning about a hundred new cases hospitalized. Saturday the 10th infection results will be out this afternoon.
The reduction of the infection rate by almost a full percent over three days is positive despite the 1,483 covid infections (because more persons were tested) is significant.
The troubling factor is how spreading of disease, either through Covid-19 or the new variant highlighted by Governor Andrew M. Cuomo Friday is that the spread of the disease has spread ominously to the more lightly populated suburbs which are fueling the infection rate by no enforcement whatsoever accept voluntary restrictions recommended by the County Department of Health.
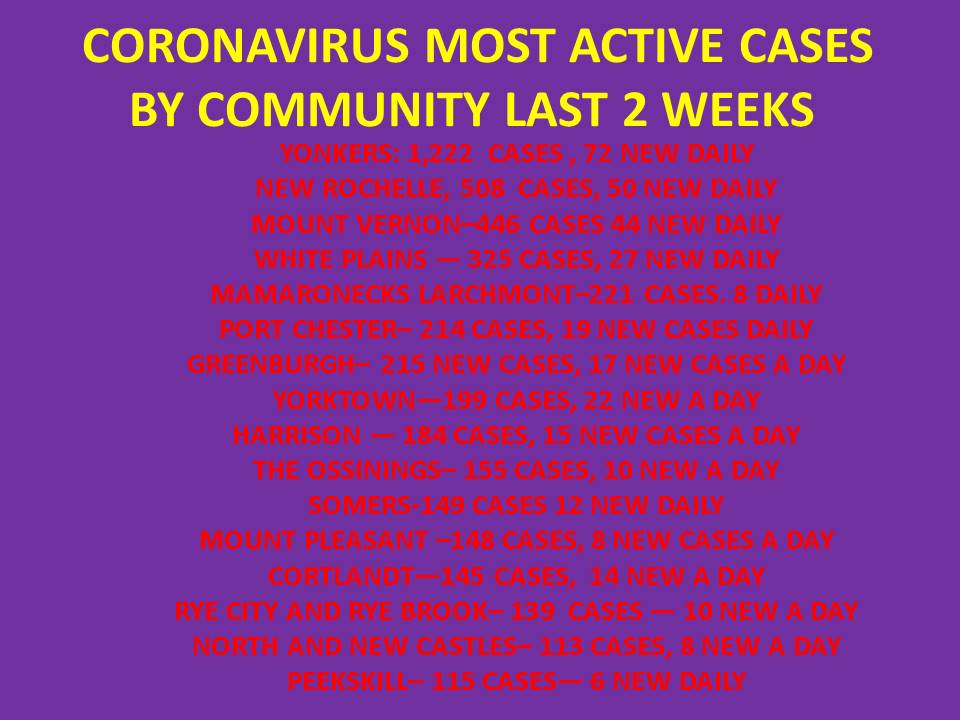
Notice the town by town figures on infections the past two weeks compiled by WPCNR from the Westchester County Covid Tracker by towns and cities. The town infections are rising.
THE NEW VARIANT B.1.1.7 PROFILE bY Dr. Sanjay Mishra.
The following article by Dr. Sanjay Mishra, Mishra, a child psychiatrist in Carmel, Ind., and a partner and medical director of Indiana Health Group, a large medical practice specializing in mental health was circulated to WPCNR.
This article appeared in Saturday’s edition of National Geographic and appears on the NG website. Dr. Mishra delves into the reasons why the new variant arriving in New York is perhaps more serious than the first Covid, requiring continued covid precaution:
“The coronavirus variant known as B.1.1.7, which studies show is both more deadly and more transmissible than the original version of SARS-CoV-2, is now the most common strain circulating in United States, and its growing prevalence has alarmed prominent epidemiologists.
Earlier in the pandemic, not many children were becoming infected with the coronavirus, and they did not appear to be major sources of virus transmission to other age groups. “That changed with B.1.1.7,” says epidemiologist Michael Osterholm, director of the Center for Infectious Disease Research and Policy. “We’re now seeing substantial numbers of outbreaks in schools and in school-related activities.”
In a study conducted in the U.K., where this variant was first detected, more children were infected with B.1.1.7 than other SARS-CoV-2 variants, compared to older age groups. The same scenario is now emerging in the U.S.
A rapidly growing outbreak of COVID-19 in Carver County, Minnesota, has been linked to school-sponsored and club sports activities. In a study done by the Minnesota Department of Health, researchers produced a detailed map of COVID-19 transmission showing that the B.1.1.7 variant caused about a quarter of these cases. A similar outbreak was reported in Wisconsin, where all the children at a Dane County childcare center who tested positive were 6 years or younger.
The upside, if there is one, is that one study suggests younger children were less likely than adults to pass the virus to others. In addition, the current vaccines authorized for use in the U.S. are effective against B.1.1.7 and can help us reverse the course of the pandemic, as long as people also continue to limit exposure by following the current public health precautions and restrictions.
“If you need another reason to get vaccinated, here it is,” says William Schaffner, a physician and professor of infectious diseases at Vanderbilt University Medical Center. “Not only is it more contagious, but when you are infected with it, you’re more likely to get serious disease. And so we’re concerned about it.”
A more contagious virus enters the U.S.
In early December, as optimism was rising about the U.K.’s ambitious vaccine rollout, British scientists and public health officials were seeing a surge of cases in Kent County in southeastern England. While only 4 percent of those cases were sequenced, almost half were found to be the new variant of SARS-CoV-2.
Because this variant, now called B.1.1.7, is much more contagious, it spread quickly worldwide, and by December 29 the Colorado Department of Public Health & Environment reported the first case in the U.S. However, several studies have now shown that B.1.1.7 likely entered the U.S. multiple times between November 2020 and January 2021—earlier than previously thought.
In early February, Karthik Gangavarapu, a graduate student at The Scripps Research Institute in La Jolla, California, co-authored a study that predicted B.1.1.7 would become dominant in the U.S. by late March 2021.
“Based on what we had seen in other parts of the world with this variant, there was no reason for us to believe that this wouldn’t happen in the U.S., and I think, for most epidemiologists, this is not a huge surprise,” Gangavarapu says.
Currently in U.S., the number of cases caused by B.1.1.7 is increasing at a rate of about 7.5 percent per day.
Researchers believe the variant spreads so rapidly because B.1.1.7 accumulated a large number of genetic changes—17 in total—including eight in the virus’s hallmark spike protein. The spike protein attaches to the ACE2 receptor protein, which is found on the outer wall of 72 types of human cells. After the virus latches onto the ACE2 receptor, it can enter the host cell, make more copies of itself, and trigger infection.
By binding more tightly to the ACE2 receptors, “these mutations provide selective advantage to B.1.1.7, so that’s why now it is spreading everywhere” says Olivier Schwartz, head of the Virus and Immunity Unit of the Pasteur Institute in Paris, France. “It’s a kind of a Darwinian selection process.”
A study analyzing more than 100,000 people who had been infected with either B.1.1.7 or the original strain also shows that the new variant is more deadly.
When the researchers compared the two groups of patients, B.1.1.7 had greater mortality by somewhere between 32 and 104 percent, says team leader Robert Challen, a clinician at the University of Exeter in the U.K.
Some researchers believe that B.1.1.7 behaves so differently from the original strain that it can even be “treated as a separate epidemic,” says Ravindra Gupta, a professor of clinical microbiology at the University of Cambridge.
B.1.1.7 also been causing problems in other ways. It carries a couple of genetic mutations in the spike protein called deletions, because they eliminate part of the genetic code, that help this variant escape antibodies during the body’s immune response after an infection.
These deletions can also cause certain commercial testing kits to give a false negative result because they fail to detect its spike protein gene. The U.S. Food and Drug Administration has issued recommendations to address possible false negative results that arise due to increasing prevalence of B.1.1.7 and other deletion variants in the U.S.
Implications for kids
The risk of B.1.1.7 to children, and subsequently to their families, may not arise as much from higher transmissibility, but from kids’ inability to maintain social distancing and masking and avoid contact sports, says Osterholm.
According to Schwartz, since the virus is more infectious for all age groups, children can now get infected more easily because of close contact in schools and day care. Then they can transmit more virus to each other, and to their families at home.
Because of increasing demand to reopen schools, there is now higher transmission of the B.1.1.7 variant among kids. That means more schools will have difficulty maintaining in-class learning.
The good news is that people who have been vaccinated, or people who were previously infected with another variant, have antibodies that will still neutralize B.1.1.7, says Schwartz, who led a study showing this to be the case. Already, vaccine makers are releasing clinical data showing that the available shots protect children age 12 to 15, and studies in younger children are forthcoming.
“The challenge is we’re not going to have nearly enough vaccine fast enough” to rein in the pandemic unless people stick to safety restrictions in the meantime, Osterholm lamented. “If we don’t limit our exposures to this virus, and try to defy viral gravity, we will not be able to do that.”